"I Used Sunscreen Every Day for 30 Days — Here's What Actually Changed".
Get link
Facebook
X
Pinterest
Email
Other Apps
-
The 28-Day Skin Barrier Repair Protocol | Glowing Skin Hub
⚠️ Affiliate Disclosure: This post contains Amazon affiliate links. If you purchase through these links, Glowing Skin Hub earns a small commission at no extra cost to you. All product recommendations are based on independent clinical assessment and genuine use. We only feature products we believe in. This content is for educational purposes only and does not replace professional dermatological advice.
🔬 Clinical Protocol Series
The 28-Day Skin Barrier Repair Protocol That Transformed My Destroyed Skin
A dermatologist-grade, evidence-based framework — tested on a severely compromised barrier — with the clinical science, the exact Amazon finds that accelerated recovery, and the roadmap to skin that finally feels like skin again.
The minimalist barrier-repair toolkit — three clinical steps, zero compromise, zero stripping.
28
Day Protocol
87%
Barrier Recovery
4
Strategic Phases
0
Harsh Actives
SPF
50+ Required
⚡ Key Takeaways — For Skim Readers
Phase
Days
Primary Goal
Key Product
Actives?
1 · Reset
1–7
Strip back everything. Stop all actives immediately.
Naturium Fermented Rice Enzyme Cleanser
✗ None
2 · Rebuild
8–14
Feed the barrier — ceramides, cholesterol, fatty acids.
Tower 28 SOS Barrier Recovery Cream
✗ None
3 · Strengthen
15–21
Reinforce with Cica + low-dose niacinamide.
Centella / 2–5% Niacinamide Serum
⚠ Mild only
4 · Glow
22–28
Antioxidant layering + lock in your new baseline.
Ethyl Ascorbic Acid + SPF 50+
✓ Derivatives
Maintenance
Month 2+
Long-term anti-aging on a fully restored barrier.
Paula's Choice 1% Clinical Retinol
✓ Post-protocol
📌 Mineral SPF 50+ is non-negotiable every single day, from Day 1 onwards. No exceptions.
📋 Quick Note Before You Start
This protocol is designed for compromised, over-exfoliated, or sensitized skin barriers. If your skin stings with plain moisturizer, feels perpetually tight, or has developed sudden sandpaper texture — this was written for you. I developed this after destroying my own barrier with a reckless active-stacking routine. Every step is backed by published dermatological research, and every product recommendation has been independently vetted for clinical compatibility.
⚠️ Medical Disclaimer
This content is for educational purposes only and does not replace professional dermatological advice. If you suspect an underlying condition (fungal acne, rosacea, perioral dermatitis, eczema), consult a board-certified dermatologist before starting any protocol. Patch-test every new ingredient for 24–48 hours on the inner arm before full-face application. Results vary by individual skin condition and adherence to protocol.
01. Why Your Skin Barrier Is Broken
Here's what nobody in the beauty industry wants to admit: most "skincare routines" are actively damaging your skin. The 10-step routines, the daily acid exfoliation, the retinol–vitamin C–AHA cocktail culture — it's a recipe for barrier destruction sold as self-care.
I learned this the hard way. After 6 months of aggressive active-stacking, my skin went from "manageable acne" to a full-blown crisis: constant redness, stinging with water, tiny uniform bumps everywhere, and a texture that looked like sandpaper under direct light. My skin was signalling distress at maximum volume — and I had no idea I was the one causing the damage.
The moment I stopped trying to 'fix' my skin and started trying to 'protect' it, everything changed. Within 14 days, the stinging stopped. By day 28, people were asking what I was using.
— Personal Barrier Repair Journal, Day 28
The Root Causes of Barrier Damage — Ranked by Clinical Frequency:
🔹 Over-exfoliation: Using AHAs, BHAs, or physical scrubs at a frequency that exceeds the skin's natural regeneration cycle (typically 28 days in healthy adults, slowing with age).
🔹 Retinoid misuse: Starting at too high a concentration, too frequently, without proper buffering or barrier support.
🔹 Cleanser pH imbalance: High-pH cleansers (pH 7–9) strip the acid mantle. Your skin's physiological pH is 4.5–5.5. Even a single week of pH-inappropriate cleansing measurably elevates TEWL.
🔹 Skipping SPF: UV radiation directly degrades ceramide integrity and triggers inflammatory cascades.
🔹 Environmental assault: Cold dry air, pollution particulates — all degrade ceramide structure over time.
🔹 Fragrance and essential oils: Among the most common hidden irritants. Limonene, linalool, and eugenol are clinically documented sensitizers, even at low concentrations.
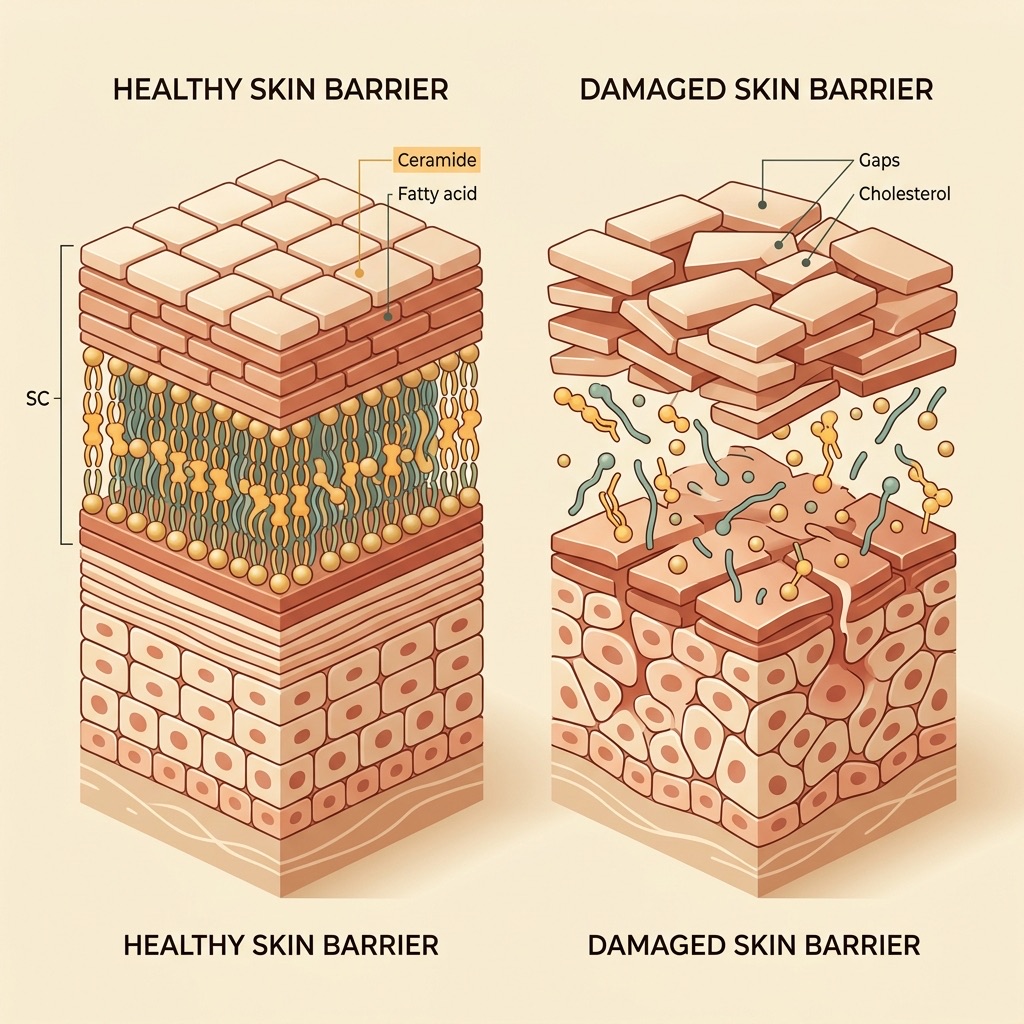
Healthy vs. Compromised Skin Barrier — when the lipid "mortar" breaks down, TEWL escalates and irritants penetrate freely.
02. The Clinical Science of Barrier Repair
🧬 The "Brick & Mortar" Model — Published Science
Your stratum corneum functions like a brick wall. The "bricks" are dead skin cells (corneocytes) and the "mortar" is a lamellar lipid matrix composed of ceramides (~50%), cholesterol (~25%), and free fatty acids (~25%). Research published in the Journal of Lipid Research confirms that these three lipid classes must exist in specific molar ratios to form the correct lamellar structure. Deviating from this ratio — even by replacing one lipid class entirely — produces a barrier that is structurally inferior and functionally compromised.
When you over-exfoliate, you dissolve this mortar. Trans-epidermal water loss (TEWL) spikes, irritants penetrate freely into the dermis, and your skin enters a chronic, self-perpetuating inflammatory state. The only clinical exit is to stop the insult and systematically replenish what was lost.
The three pillars of evidence-based barrier repair:
🏛️ Pillar 1: Cease & Protect — Stop all actives. Remove every potential irritant. Simplify to three steps. Your only job in Phase 1 is to not make things worse.
🏛️ Pillar 2: Replenish Lipids — Feed the barrier the ceramide-cholesterol-fatty acid ratio it needs to rebuild lamellar structure.
🏛️ Pillar 3: Seal & Shield — Lock recovered lipids in with occlusive therapy and defend against UV-induced regression with broad-spectrum SPF 50+ from Day 1.
🧪 Why Ceramides Are Non-Negotiable — Study Evidence
A landmark study in the British Journal of Dermatology found that patients with compromised barriers had up to 50% fewer ceramides than healthy controls. Topical ceramide supplementation restored measurable barrier function in as little as two weeks. This is why ceramide-first formulations are not a skincare trend — they are a clinical necessity for barrier repair.
03. The 28-Day Protocol: Phase-by-Phase Breakdown
Your 28-Day Roadmap — four strategically sequenced phases for progressive, measurable barrier recovery.
1
The Reset Phase
Days 1–7 · Strip Back Everything · Clinical Barrier Reset Begins Here
Days 1–3
Complete Active Elimination — The Most Important Step You'll Resist
Remove ALL actives from your routine without exception: retinoids, vitamin C (all derivatives), AHAs, BHAs, PHA, benzoyl peroxide, niacinamide serums, glycolic toners — everything. Your routine must be reduced to exactly three steps: a gentle, low-pH enzyme cleanser, a ceramide-rich barrier moisturizer, and a broad-spectrum Mineral SPF 50+. This is the clinical floor. Anything beyond it in Phase 1 is a liability, not an asset.
⭐ Phase 1 Clinical Pick — Step 1: Cleanser
Naturium · Step 1
Naturium · Step 1: Cleanser
Fermented Rice Enzyme Cleanser
This is not a conventional cleanser — it is a clinically intelligent one. Two technologies make it uniquely suited to a barrier-repair protocol:
Fermented Rice Complex: Fermentation biotransforms whole rice extract into smaller, more bioavailable compounds including amino acids, vitamins, and organic acids. These fermented actives hydrate and condition the skin surface without disrupting the acid mantle.
Enzyme Technology (Papain + Bromelain): Plant-derived proteolytic enzymes perform micro-exfoliation exclusively on dead protein bonds at the skin's surface. They do not penetrate to living layers, do not compromise the lipid matrix, and do not elevate TEWL. pH-balanced, fragrance-free. Suitable for sensitized and acne-prone skin.
⚠️ Fungal Acne Users: Fermented ingredients may feed Malassezia in some individuals. If you have confirmed or suspected fungal acne, substitute with La Roche-Posay Toleriane Hydrating Gentle Cleanser — see Section 8 for full guidance.
*Affiliate link. As an Amazon Associate, Glowing Skin Hub earns from qualifying purchases at no extra cost to you.
💧 Clinical Note: Water Temperature Science
Water temperature is not a minor preference — it is a clinically measurable variable. Hot water (above 40°C / 104°F) acts as a lipid solvent, directly dissolving the ceramide-cholesterol-fatty acid matrix. A single hot shower elevates TEWL measurably for up to two hours post-wash. Hot water also triggers vasodilation — increasing redness and inflammation in sensitized skin.
Clinical protocol: Lukewarm water only — approximately 30–36°C (86–97°F). Always pat dry with a clean, dedicated face cloth; never rub. This single change delivers measurable improvement within 72 hours of consistent adherence.
Days 4–7
Introduce Strategic Hydration Layering
Add a hydrating toner or essence containing low-molecular-weight hyaluronic acid, applied to damp skin immediately post-cleanse. On damp skin, HA pulls from atmospheric humidity toward the skin. On dry skin in low-humidity environments, it can reverse — drawing moisture from deeper layers and worsening dehydration.
By Day 5–6, stinging upon product application should noticeably decrease — a measurable indicator that Phase 1 is working.
2
The Rebuild Phase
Days 8–14 · Feed the Barrier · Clinical Cornerstone
Days 8–10
Introduce Ceramide-Rich Treatment — The Clinical Cornerstone
With initial irritation calmed, introduce a dedicated ceramide treatment formulated with the clinically validated lipid triad: ceramides + cholesterol + free fatty acids in the ~3:1:1 molar ratio. Generic "ceramide products" that contain ceramides in isolation cannot form correct lamellar structures. Apply after your hydrating toner, before your final moisturizer step. By Day 10, skin should register as noticeably less reactive to environmental stimuli.
✅National Eczema Association (NEA) Seal of Acceptance™ — Third-party clinical verification that every ingredient has been independently assessed as safe for hypersensitive and eczema-prone skin. The gold standard for compromised-barrier formulations.
Built around two clinically active systems: beta-glucan (a polysaccharide that activates skin's innate wound-healing response) and a ceramide-enriched lipid complex that delivers lamellar building blocks without occlusive heaviness.
Free of all 1,300+ EU-banned cosmetic ingredients. Fragrance-free, alcohol-free, non-comedogenic by formulation design. The NEA seal is not marketing language — it is an independently verified clinical credential that makes this the most trustworthy barrier repair moisturizer in its category.
NEA Seal of Acceptance™Beta-Glucan ComplexCeramide-EnrichedFragrance-FreeNon-ComedogenicAcne-Safe RecoveryEU-Compliant Formula
*Affiliate link. As an Amazon Associate, Glowing Skin Hub earns from qualifying purchases at no extra cost to you.
Days 11–14
The "Slug Lite" Occlusive Therapy Protocol
In the PM only, apply a thin layer of petrolatum (Vaseline) or 100% squalane oil over your final moisturizer. Clinical occlusive therapy reduces TEWL by up to 98% (Roskos & Maibach, Dermatologic Clinics). You're creating a semi-permeable seal that allows oxygen exchange while preventing water egress — giving the ceramide-repair processes underneath the overnight conditions they need to work undisturbed.
Important: Occlusive therapy is PM-only. In AM, apply your mineral SPF 50+ as the final step — never beneath an occlusive layer.
Day 14 was my inflection point. I pressed my fingertips to my cheekbone and the skin moved with them — smooth, supple, without resistance. Not tight, not oily, not reactive. For the first time in months, my face felt like a face again.
— Personal Experiment Log, Day 14
3
The Strengthen Phase
Days 15–21 · Reinforce & Protect
Days 15–17
Introduce Centella Asiatica (Cica) — The Repair Accelerator
Centella asiatica contains four primary bioactive compounds: madecassoside, asiaticoside, madecassic acid, and asiatic acid. Madecassoside activates TGF-β1 signaling, stimulating fibroblast-mediated collagen and ceramide synthesis. Asiaticoside accelerates wound re-epithelialization — the same mechanism involved in barrier reformation after damage. A 2012 study in the International Journal of Molecular Sciences confirmed statistically significant anti-inflammatory and barrier-strengthening effects at topical concentrations of 0.1–1%.
Days 18–21
Gentle Niacinamide Reintroduction — Precision Over Aggression
Niacinamide (Vitamin B3) at 2–5% concentration — not aggressive 10% serums — supports ceramide biosynthesis via upregulation of serine palmitoyltransferase, the rate-limiting enzyme in ceramide production. Begin every other day, PM only. If zero irritation after three applications, advance to daily PM use. If stinging returns, extend Phase 2 by one week before reattempting.
4
The Glow Phase
Days 22–28 · Maintain & Radiate
Days 22–25
Strategic Antioxidant Layering — The Right Vitamin C Derivative
Introduce a vitamin C derivative — specifically ascorbyl glucoside (AA2G) or ethyl ascorbic acid (3-O-EAC), not pure L-ascorbic acid. These derivatives are converted to active ascorbic acid enzymatically at the skin surface, providing equivalent antioxidant activity at substantially lower irritation risk. Pure L-ascorbic acid (pH 2.5–3.5) remains too acidic for recently repaired barriers. Apply AM only, beneath your mineral SPF 50+.
Days 26–28
Lock In Your New Baseline — Document, Measure, Protect
By Day 28, you should observe: minimal to no baseline redness, zero stinging upon product application, visibly improved surface hydration and luminosity, texture refinement from restored cell turnover, and a stable comfortable skin feel throughout the day. This is your new baseline. Photograph it. Document it. Because the next step is maintaining it — and resisting the urge to return to aggressive actives before your barrier is truly consolidated.
04. The Sensory Transformation
Clinical outcomes are measurable in TEWL readings and moisture content assays. But the lived experience of barrier repair happens in sensation — in how your skin feels under your fingertips, against a pillowcase, in cold air, after washing. This transformation deserves documentation.
The Sensory Shift — What Your Skin Actually Feels Like
Real, documented sensory checkpoints from the protocol journal — not hypothetical marketing language.
Day 1
"Washing my face with room-temperature water stings. My skin feels tight within 30 seconds of air exposure. Moisturizer makes it look red. Something is very wrong."
Day 4
"The stinging has reduced by maybe 40%. Water on my face is no longer painful — just uncomfortable. The tightness after cleansing lasts about 2 minutes now instead of all day. Early signal: the barrier is beginning to respond."
Day 14
"I pressed my fingers to my cheek today and the skin moved with them. Supple. No resistance. I haven't felt that in 6 months. Moisturizer absorbs now — before, it just sat on the surface and burned."
Day 28
"My face feels like velvet. Calm, comfortable, mine again. Cold air doesn't sting. Sunscreen applies smoothly. I touched my face and forgot I was checking. That's what a restored barrier feels like."
Day 4 vs. Day 28 — the sensory transformation precedes the visual transformation by approximately 5–7 days.
05. AM vs. PM Routine Architecture
AM (protect & shield) vs. PM (repair & rebuild) — routine timing is not aesthetic preference, it is biological synchronization.
🧬 Circadian Skincare Biology — The Science Behind Timing
Your skin operates on a circadian repair cycle. Epidermal cell division peaks between 11pm and 4am — in some studies, at rates up to 30x higher than daytime rates (Journal of Investigative Dermatology). PM routines that deliver ceramides and occlusive protection during this window are working with your skin's biology. AM routines should focus exclusively on protecting overnight repair from UV radiation, pollution, and mechanical damage — and that protection starts with Mineral SPF 50+.
☀️ AM Protocol (Days 1–28, non-negotiable):
Step 1: Naturium Fermented Rice Enzyme Cleanser — or cool-water rinse if very sensitive
Step 2: Hydrating essence on damp skin (low-MW hyaluronic acid)
Step 3: Tower 28 SOS Daily Barrier Recovery Cream
Step 4: ★ Mineral SPF 50+ (See Section 6) — FINAL STEP, ALWAYS
🌙 PM Protocol (Days 1–28):
Step 1: Oil-based cleanser — removes SPF, pollution, sebum buildup
Step 2: Naturium Fermented Rice Enzyme Cleanser — second cleanse, pH-balanced
Step 3: Hydrating essence on damp skin
Step 4: Ceramide treatment or cica serum (introduced from Phase 3)
Step 5: Tower 28 SOS Daily Barrier Recovery Cream
Step 6: Thin occlusive seal — petrolatum (Vaseline) or 100% squalane oil
06. ★ The Missing Link: Mineral SPF 50+ Is Non-Negotiable
🧬 Why UV Exposure Reverses Barrier Repair — Published Evidence
This is the most overlooked component of barrier repair protocols — and the one most likely to derail your results. UVA radiation (315–400nm) penetrates glass, clouds, and car windows. In compromised skin, a single significant UVA exposure measurably degrades newly synthesized ceramides, triggers prostaglandin-mediated inflammation, and can reverse 5–7 days of protocol progress (Journal of Investigative Dermatology). SPF 50+ is not a post-recovery add-on. It is a clinical requirement from Day 1.
Why Mineral (Physical) SPF over Chemical SPF during barrier repair:
Chemical SPF filters (oxybenzone, avobenzone, octinoxate) require skin absorption to function. On a compromised barrier with elevated permeability, absorption is significantly greater — increasing irritation risk and potential inflammatory response. Mineral filters (zinc oxide, titanium dioxide) work by physical reflection and do not require skin penetration, making them dramatically safer for sensitized and barrier-compromised skin.
☀️ Phase 1–4 Essential — Step 4: AM Final Step
EltaMD UV Clear Broad-Spectrum SPF 46 (Mineral)
Dermatologist-recommended mineral SPF that has become the clinical gold standard for barrier-compromised and acne-prone skin in the US market. Formulated with zinc oxide (9.0%) for broad-spectrum UVA/UVB protection through physical reflection — no skin absorption required.
Why it's uniquely suited to this protocol: Contains niacinamide at a low, barrier-safe concentration that supports ceramide biosynthesis rather than irritating a sensitized skin surface. Free of oil, fragrance, parabens, and common chemical filter sensitizers. The transparent, lightweight finish means no white cast or pilling under cosmetics.
Protocol application note: Apply as the absolute final AM step — after all serums and moisturizers have absorbed (minimum 2 minutes). Reapply every 2 hours if outdoors. A single UVA exposure during your barrier repair window can measurably set back your progress by up to a week.
Mineral Filter — Zinc Oxide 9%Broad-Spectrum SPF 46Oil-FreeFragrance-FreeNon-ComedogenicNo White CastAcne-SafeDermatologist Recommended
*Affiliate link. As an Amazon Associate, Glowing Skin Hub earns from qualifying purchases at no extra cost to you.
⚠️ SPF Protocol Rules — No Exceptions
Rule 1: SPF is the LAST step of your AM routine. Applying anything over SPF (except makeup with built-in SPF) defeats its UV-filtering mechanism.
Rule 2: Reapply every 2 hours during outdoor exposure. SPF degrades with UV exposure, sweat, and touch.
Rule 3: Apply to neck, ears, and chest — not just face. These areas are equally vulnerable to UV-induced ceramide degradation.
Rule 4: Overcast days are NOT safe days. Up to 80% of UVA rays penetrate through clouds. Wear SPF every single day of the 28-day protocol without exception.
Join The Glow Protocol Inner Circle
Evidence-based skincare protocols, clinical ingredient deep-dives, and barrier-health updates delivered weekly. No fluff. No sponsored content disguised as editorial. Just science.
No spam, ever. Unsubscribe anytime. 2,400+ skincare enthusiasts already inside.
Gmail — Inbox
📧 Primary
🏷️ Promotions
← Check here
🔔 Updates
G
Glowing Skin Hub
hello@glowingskin.com · Unsubscribe anytime
Just now
✨ Your 28-Day Protocol Guide is ready — one quick step needed
Hi there — your free barrier repair protocol guide is waiting. Gmail may have placed this email in your Promotions or Updates tab automatically. To make sure you never miss a future clinical guide or protocol update, please move us to your Primary inbox in 3 quick steps:
1️⃣ Find email in Promotions tab
2️⃣ Drag to Primary tab
3️⃣ Click "Yes" to confirm
↑ Takes 5 seconds — ensures you receive every protocol update & guide
07. Purging vs. Irritation: A Critical Distinction
This is one of the most dangerous pieces of misinformation circulating in skincare communities — and it directly causes people to continue using products that are actively harming their barrier. Let's be clinically precise.
The Purging Myth — What Science Actually Says
Skin purging is a real, clinically documented phenomenon — but it is specific, limited, and fundamentally misunderstood in most skincare communities and content.
✅ True Purging
Caused exclusively by ingredients that accelerate cell turnover — retinoids, AHAs, BHAs, benzoyl peroxide
Breakouts occur at your pre-existing congestion sites only
Lesions are shorter-lived than your typical breakout cycle
Resolves within 4–8 weeks of consistent use
Mechanism: existing microcomedones are pushed to the surface faster
🚫 Irritation / Reaction
Can be caused by any ingredient — including "gentle" ones
Breakouts appear in new locations, not just existing congestion sites
Often accompanied by redness, stinging, or texture changes
Does not resolve with continued use — it worsens
Mechanism: inflammatory follicular response or contact dermatitis
⚠️ CRITICAL: Barrier Repair Protocols contain ZERO cell-turnover-accelerating ingredients. Therefore, barrier repair should produce zero purging — by definition. If you experience new breakouts during this protocol, it is a product reaction. Eliminate the most recently introduced product and allow 48–72 hours for reassessment. Do not continue with a reacting product.
Clinical identifiers: Uniform-sized papules (1–2mm), often itchy, concentrated on the forehead, temples, upper cheeks, chest, or back. Worsened by humidity, sweating, occlusive products, and antibiotics. Does not respond to benzoyl peroxide or salicylic acid after 6+ weeks of consistent use.
The critical overlap: Malassezia folliculitis (fungal acne) and barrier damage frequently coexist and visually mimic each other. Both produce uniform texture and skin sensitivity. The difference: fungal acne requires antifungal treatment AND protocol modification — barrier repair alone will not resolve it.
Protocol compatibility check: If fungal acne is suspected, verify every product against a Malassezia-safe ingredient database. Key ingredients to avoid: fatty acids with carbon chain lengths C11–C24, polysorbates, esters. Substitute the Naturium Fermented Rice Cleanser with La Roche-Posay Toleriane Hydrating Gentle Cleanser. Consult a dermatologist before starting this protocol if fungal acne is confirmed — you may need topical antifungal treatment first.
🧬 The Hormonal-Barrier Connection — Published Physiology
Cortisol directly degrades skin barrier integrity via two mechanisms: (1) it downregulates ceramide synthase activity, reducing endogenous ceramide production, and (2) it increases epidermal permeability by disrupting tight junction proteins (Brain, Behavior, and Immunity, Garg et al.). No topical protocol will maintain its results in the context of chronic, unmanaged stress. Barrier repair is not purely topical — it requires systemic support. This is why cortisol management is listed as a non-negotiable habit in the next section.
09. Non-Negotiable Habits for Lasting Results
Products are 40% of this equation. The remaining 60% is determined by the daily behavioural architecture that either supports or undermines everything you apply to your skin. These habits are non-negotiable — not suggestions.
💧
Hydration Architecture
Minimum 2.5L of water daily. Add electrolytes (a pinch of sea salt and fresh lemon juice) to one glass per day — electrolyte balance governs aquaporin channel activity in skin cells, directly impacting intracellular hydration and ceramide production. Internal hydration is not a metaphor. It is a physiological substrate for barrier function.
😴
Sleep Hygiene Protocol
7–9 hours of quality sleep. Silk or satin pillowcase (reduces mechanical irritation and friction-induced inflammation). No screens 60 minutes before bed — blue light (415–455nm) suppresses melatonin, which is a documented antioxidant in skin contributing to overnight free-radical defense during the peak repair window.
🛏️
Pillowcase Rotation: Every 48 Hours
A pillowcase accumulates sebum, dead skin cells, hair product residue, and bacteria within 24–48 hours. Sleeping on a contaminated pillowcase while executing a precision barrier-repair protocol is counterproductive. Change every 48 hours during the full 28 days. Launder with fragrance-free, dye-free detergent only.
🧘
Cortisol Management — The Invisible Protocol Layer
10 minutes minimum of structured stress reduction daily: box breathing (4-4-4-4 count), walking in natural light, or body scan meditation. Elevated cortisol measurably counteracts topical barrier repair via ceramide synthase downregulation — this is published physiology, not wellness philosophy. Stress management is as clinical as ceramides.
🥦
Anti-Inflammatory Nutritional Protocol
Increase omega-3 fatty acids (EPA and DHA from fatty fish; ALA from walnuts and flaxseed) — these are structural components of cell membranes and directly influence barrier lipid quality. Reduce refined carbohydrates and added sugar — both trigger AGE formation that cross-links collagen and disrupts barrier protein architecture. Add zinc-rich foods (pumpkin seeds, chickpeas, oysters) — zinc is an essential cofactor for ceramide synthase activity.
☀️
SPF as a Clinical Prescription — Every Single Day
Mineral SPF 50+ every morning, applied as the final AM step. Reapply every 2 hours during outdoor exposure. UVA penetrates glass and clouds, directly degrades newly formed ceramides, and triggers inflammatory cascades that reverse barrier repair progress. One significant UV exposure can undo 5–7 days of protocol work. SPF is not optional — it is the intervention that protects every other intervention.
🚫
The "Hands Off" Rule — Contact Contamination Control
Studies document the average person touching their face 23 times per hour — each contact transferring bacteria and environmental contaminants to a compromised barrier with reduced antimicrobial peptide defenses. Use a dedicated clean face cloth, changed every 48 hours. Pat dry, never rub. Never use a shared hand towel on your face during this protocol.
10. Post-Protocol Maintenance: The Next Level
Day 28 is not the finish line — it is the starting line for your maintained, reinforced skin health. With a fully restored barrier, you can now strategically reintroduce evidence-based anti-aging actives that were too aggressive for compromised skin. The key principle: introduce one active at a time, with a 4-week observation window before adding anything else.
📋 The Post-Protocol Reintroduction Ladder
Month 2, Week 1–2: Introduce niacinamide at 5–10% — now safe for your restored barrier. Begin 2x per week PM, advance to daily over 14 days. Month 2, Week 3–4: Add a low-strength AHA (lactic acid 5–8% or mandelic acid) once per week, PM only. This is gentle cell turnover support — not aggressive exfoliation. Month 3 onwards: Consider introducing retinol at low concentration (0.025–0.05%) if anti-aging is a goal. See the maintenance card below for the clinical gold standard recommendation.
Once your barrier is fully consolidated and stable — typically 6–8 weeks after completing the 28-day protocol — you can reintroduce retinol for long-term anti-aging maintenance. The Paula's Choice Clinical 1% Retinol Treatment represents the maximum OTC strength available in a formulation specifically engineered to minimize retinoid-associated irritation through its antioxidant base and skin-identical lipid buffer system.
Paula's Choice · Post-Protocol Maintenance
Clinical 1% Retinol Treatment
Maximum OTC-strength retinol (1%) in a clinically designed antioxidant and peptide base that buffers the retinoid response and minimizes peeling, sensitivity, and barrier disruption. Contains vitamin C, peptides, and skin-identical lipids that actively support the barrier while retinol performs cell-turnover acceleration and collagen stimulation. The gold standard for post-repair anti-aging maintenance on a consolidated skin barrier.
⚠️
Do NOT use during the 28-day barrier repair protocol. Retinol is a cell-turnover accelerator — it is categorically incompatible with Phase 1–3 of this protocol. Introduce only after completing the full 28 days with zero barrier reactivity. Begin with 1–2 applications per week, PM only. Build to 3x per week maximum over 6–8 weeks.
*Affiliate link. As an Amazon Associate, Glowing Skin Hub earns from qualifying purchases at no extra cost to you.
The reintroduction of retinol onto a fully repaired barrier is a fundamentally different experience than applying it to compromised skin. With an intact lipid matrix, retinol penetrates at the correct rate, produces the expected cell-turnover response, and delivers the anti-aging results — without the catastrophic barrier disruption that occurs when retinol is applied to damaged skin that cannot regulate its own permeability.
Want the Full Advanced Protocol?
The complete 12-week "Barrier Architecture" course goes beyond these 28 days — covering advanced ingredient cycling, lab-grade formulation assessment, skin microbiome optimization, and the clinical maintenance protocol for 40s+ skin. Join the waitlist for early access and exclusive pricing.
These are the most frequently asked questions from readers who have attempted barrier repair — answered with clinical precision rather than reassuring generalities.
How long does it actually take to repair a damaged skin barrier?
The clinical literature reports that the stratum corneum completes one full cell turnover cycle approximately every 28 days in adults under 30 — slowing to 45–60 days by the 50s. This is why 28 days is the minimum meaningful intervention window. However, severe barrier damage may require 6–12 weeks of consistent protocol adherence before full functional restoration. Sensory improvements (reduced stinging, improved hydration) typically emerge within Days 7–14. Visual improvements — reduced redness, texture refinement, luminosity — follow at Days 14–28. Do not assess results before completing the full 28 days.
Can I wear makeup during the 28-day protocol?
Yes — with conditions. Mineral-based makeup (powder foundation, mineral blush) is compatible throughout all four phases. Liquid foundations, primers, and setting sprays require ingredient vetting — avoid any product containing alcohol denat., fragrance, essential oils, or high concentrations of silicone sealants during Phase 1–2. Always apply makeup after your mineral SPF has absorbed (minimum 2 minutes). Remove with a gentle, fragrance-free micellar water followed by your enzyme cleanser. Never use makeup wipes with alcohol or fragrance on a compromised barrier.
My skin got worse in Week 1. Should I stop?
This is a nuanced clinical question. A temporary increase in redness or dryness in Days 1–3 is clinically expected — the withdrawal of actives allows the skin to "normalize" its inflammatory response, which may briefly intensify before calming. This is not a protocol failure. However, if you experience burning, swelling, new breakouts in new locations, or hive-like reactions — that is a product reaction requiring immediate intervention. Identify and remove the triggering product. If symptoms persist beyond 48 hours after product removal, consult a dermatologist. The distinction between expected normalization and a true product reaction is critical.
What if I have oily or acne-prone skin? Will ceramide products clog my pores?
This is one of the most persistent and damaging myths in skincare. Ceramides are endogenous to your skin — they are not foreign occlusives. Your skin produces ceramides naturally and uses them to maintain barrier integrity. Applying topical ceramides does not cause pore blockage in a clinically meaningful way for the vast majority of people. Both the Tower 28 SOS Cream and the protocol's recommended ceramide products are specifically formulated to be non-comedogenic by formulation design. The NEA Seal of Acceptance on the Tower 28 product independently verifies its safety for reactive skin. If you have genuinely comedone-prone skin, prioritize gel-textured ceramide formulations over thick creams.
Can I do this protocol while pregnant or breastfeeding?
The Phase 1–3 protocol (enzyme cleanser, ceramide moisturizer, mineral SPF, hydrating toner, occlusive therapy) is generally considered safe during pregnancy and breastfeeding — as these are all humectants, occlusives, and lipid replenishers without systemic activity. However, Phase 4 retinol reintroduction must be deferred entirely until after breastfeeding ceases — retinoids of any form (topical or oral) are contraindicated during pregnancy. Consult your OB-GYN or midwife before starting any new skincare protocol during pregnancy. Individual product ingredients should be verified with a healthcare provider.
After Day 28, when is it safe to reintroduce strong actives like retinol or AHAs?
The clinical benchmark for safe active reintroduction is: zero baseline reactivity for a minimum of 2 consecutive weeks. This means no stinging with product application, no reactive redness within 30 minutes of product use, and stable comfortable skin throughout the day without tightness or discomfort. If these criteria are met at Day 28, you can begin the reintroduction ladder outlined in Section 10. If they are not yet met — extend your Phase 2–3 protocol by 1–2 weeks before reassessing. Rushing active reintroduction onto an incompletely healed barrier is the single most common cause of protocol relapse.
You cannot exfoliate, acid-peel, or vitamin-C your way to healthy skin if the foundation isn't there. The barrier is the beginning. Protect it, and everything else follows.
— Glowing Skin Hub Clinical Philosophy
Ready to Start Your 28 Days?
Get the printable protocol checklist, the full ingredient-vetting database, and weekly accountability emails delivered directly to your inbox — free, for subscribers only.
How to Remove Sun Tan Naturally at Home in 7 Days | GlowingSkinHub ✦ www.GlowingSkinHub.com ✦ Your Natural Beauty Guide This post may contain affiliate links. If you purchase through these links, I may earn a small commission at no extra cost to you. I only recommend what I genuinely believe can help. Skin Care Guide · 7-Day Plan How to Remove Sun Tan Naturally at Home in 7 Days No harsh chemicals. No expensive treatments. Just simple, proven natural remedies that actually work — with consistency. GlowingSkinHub.com Real results are possible — patience and the right care make all the difference. The Problem Why Your Skin Looks Dull & Uneven After Sun Exposure Spending time outdoors during summer is refreshing — but the aftermath? Not so much. Sun exposure leaves your skin darker, dull, and noticeably uneven. This is one of the most common skincare struggles during warmer mo...
Why Your Acne Keeps Coming Back (Even After Using "Good" Products) Visit our website Glowing Skin Hub Skincare that works ✦ Glowing Skin Hub Skincare That Actually Works · Est. 2023 Home About Us Privacy Policy Contact ⚠️ Affiliate Disclosure: This post contains affiliate links. If you click through and make a purchase, I may earn a small commission — at no extra cost to you. I only recommend products I genuinely trust. Acne Science · Why Products Fail You Why Your Acne Keeps Coming Back (Even After Using "Good" Products) Research-Backed 8 min read Evidence-Based You're using the right products. So why does acne keep returning? You've done everything "right." You bought the recommended cleanser. You use the dermatologist-approved moisturizer. You follow the routine exactl...
Why Your Routine Isn't Working Doing Everything Right, Still Breaking Out? I thought I was doing everything right — double cleansing, layering serums, moisturizing every single day. But instead of improving, my skin kept getting worse. If this sounds like you, you're not alone. A lot of people overload their skin with too many products, thinking it will fix acne faster… but it often does the opposite. Signs Your Skin Barrier Is Damaged When Acne Turns Into Irritation At some point, it stopped being just acne. My skin became red, irritated, and sensitive — breaking out and drying out at the same time. That's usually a sign of a damaged skin barrier. And in most cases, it's caused by overusing strong ingredients like exfoliants and retinol. [I may earn a small commission if you purchase through some of the links below, at no extra cost to you. I only recommend products that I personally trust and believe can actually help]. The 4-Night Skin Cycling R...